
iFR modality
(instant wave-Free Ratio)
Proven outcomes1,2,3 Superior value1,3
Philips' proprietary technology is the only resting index with with outcomes data from more than 4500 patients studied.
Introduction to the iFR modality instant wave-Free Ratio
iFR modality overview
The iFR modality Instant wave-Free Ratio:
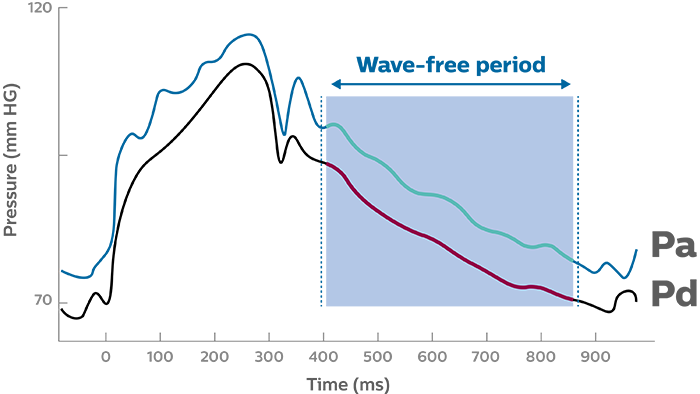
Wave-free period1
Physiology fundamentals

When resistance is constant, changes in pressure are proportional to changes in flow
Wave-free period
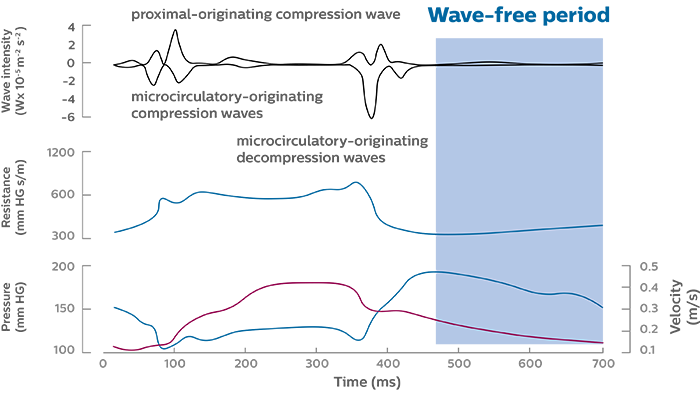
Pressure, resistance, and intensity during the wave-free period2
Benefits of the wave-free period
Case example: iFR modality with Verrata pressure guide wire in multi-vessel disease
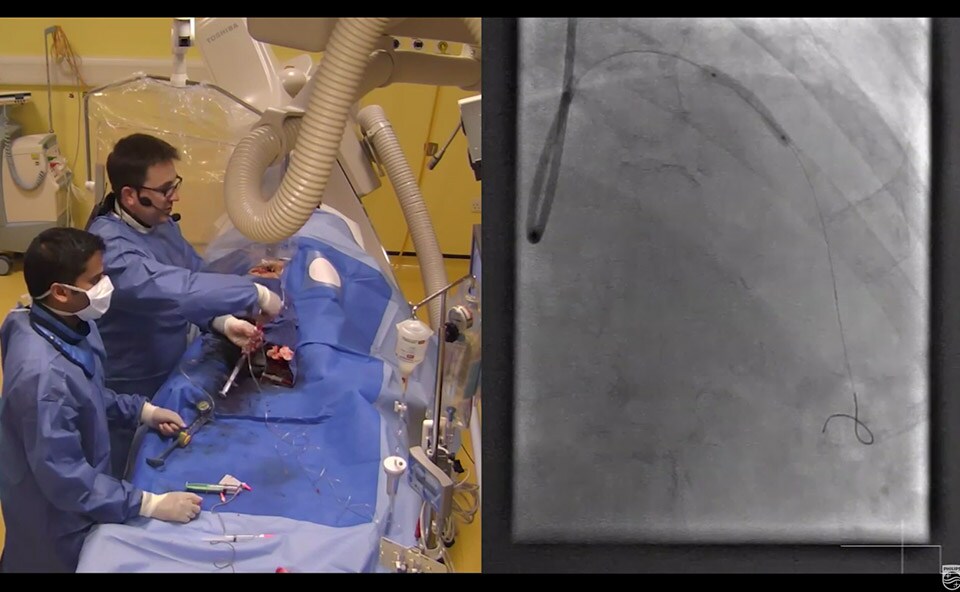
Imperial College, London - February 2014
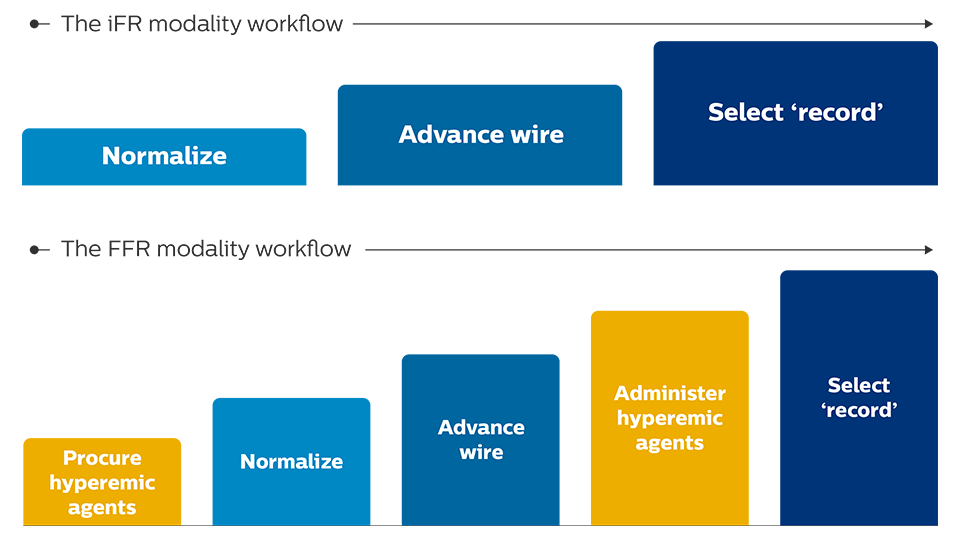
Simplifying workflow
The iFR modality provides a hyperemia-free measurement in as few as five heartbeats

Same wire, same system, fewer steps
Outcomes proven
An iFR cut-point of 0.89, single dichotomous cut-point, backed by data.1,2,6

An
Both DEFINE FLAIR and iFR Swedeheart were designed with the dichotomous cut-point of iFR in the iFR arm. With comparable MACE rates, these results mean the 0.89 cutpoint for iFR is proven and backed by more than 4500 patients of outcome.1,2
Providing choice
The Verrata Plus pressure guide wire

One wire, one system, multi-modality New in-line clip connector for improved work flow • New high fidelity sensor for reliable pressure measurement • Reliably connect and disconnect with confidence • Seamlessly switch between FFR and iFR, the only resting index with over 4500 patients studied
An iFR of 0.89 is equivalent to an FFR of 0.801,2,6
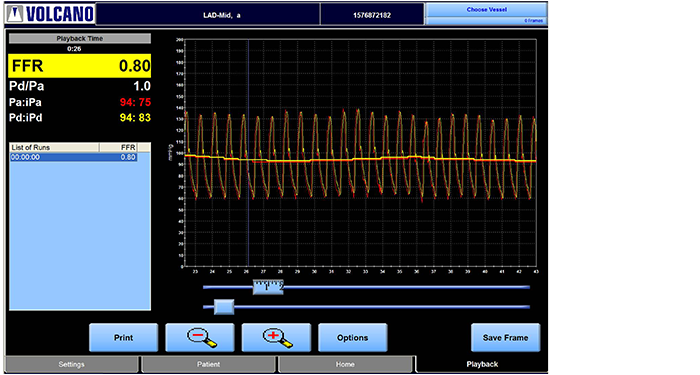
Fractional flow reserve

The iFR modality
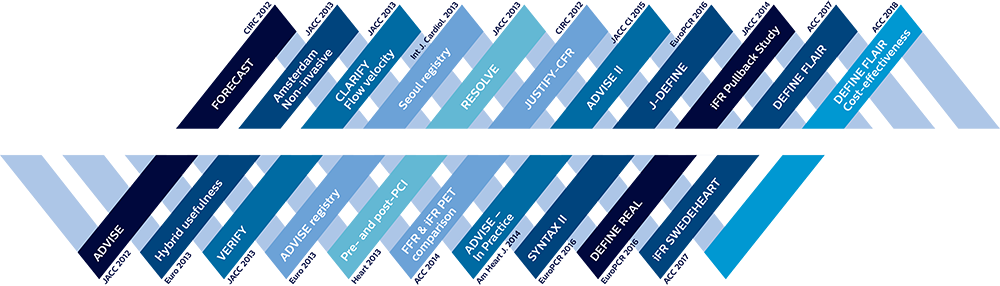
Proven outcomes
ADVISE II
DEFINE FLAIR iFR Swedeheart
Over 4000 patients have been studied with iFR and numerous prospective iFR studies have been published in peer-reviewed journals.
The two prospective, randomized, controlled trials, with more than 4500 patients' global physiology studies are Published in The New England Journal of Medicine.
Clinical articles8,9